6. Conditions affecting the oral cavity
This section is intended to broaden MCH nurses’ knowledge and recognition of oral conditions. This section describes the generally accepted practice at the time of publication. It is a guide only and as such is a general summary of the clinical knowledge. MCH nurses should use their professional judgement about applying this general information and appropriate referral to a medical professional or dental practitioner.
6.1 Gingivitis

Prevalence
Gingivitis is relatively common in children. It occurs in about half the population by four or five years of age and increases with age.
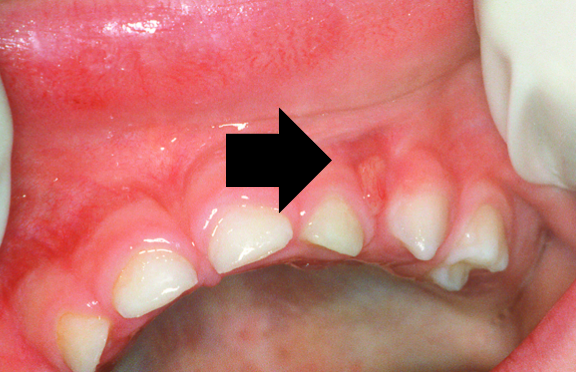
Signs and symptoms
Inflamed red gums, bleeding on touching or when soft brushing occurs, oedema (swollen gums).
Causes
Gingivitis is caused by the accumulation of plaque on the teeth and in the crevice between the gums and the teeth. Important contributors are crowded teeth and mouth breathing, which dries the gingiva
Age
Occurs in half the population by four or five years and peaks at puberty.
Duration
Totally reversible in children by improving oral hygiene.
Prevention
Good oral hygiene practices.
Treatment
Referral to a dental practitioner is required. Encourage good oral hygiene practices such as tooth brushing with a small, soft toothbrush, it is normal for the gums to bleed until gingivitis is rectified.
Gingivitis affecting the entire mouth without plaque can indicate significant systemic issues, therefore it should be referred to an dental practitioner for assessment and management.
6.2 Periodontitis
Periodontitis (meaning inflammation of the tissues surrounding the teeth) is a more severe form of gum disease affecting the deeper tissues supporting the teeth, including loss of alveolar bone.
Periodontitis in children and young people is complex and different to that seen in adults.
Periodontitis affecting adults is a slow progressive disease that can result in mobile teeth and tooth loss, and is caused by plaque. It can be worsened by smoking, diabetes. The number and severity of affected sites increases steadily with age, demonstrating that adult periodontitis can often begin in adolescent years, which is why early development of good oral hygiene is important. Periodontitis in adults responds well to improved oral hygiene.
Periodontitis affecting children and adolescents indicates other systemic issues are present. Referred to periodontitis as a manifestation of systemic disease.
Prevalence
Periodontitis in children is rare
Signs and symptoms
Periodontitis in children and adolescents can have rapid bone loss, often without significant gingival inflammation. It can result in early exfoliation of deciduous teeth with roots intact. It most commonly affects primary incisors, permanent incisors and permanent molars.
Causes
Periodontitis in children is usually a manifestation of severe systemic disease resulting in damage to the supporting tissues, these include immune deficiencies, blood dyscrasia’s and cancers, and some syndromes.
Treatment
Referral to an dental practitioner is essential if periodontitis is suspected in a child, they will then need to discuss possible underlying issues to investigate with the child’s GP or Paediatrician.
6.3 Trauma to the teeth
Trauma to a deciduous tooth can lead to fracture of the tooth itself, the tooth root or the supporting bone. It can also lead to displacement of the knocked tooth into the bone, or the tooth could be knocked out.
If a deciduous tooth is knocked out:
- do not re-implant the tooth back in the socket
- retrieve and place the tooth (or fragments) in a jar containing normal saline, the patients’ saliva or plain milk, or wrap in plastic cling wrap. Do not rinse or store in water. Do not touch the root of the tooth
- apply pressure to gum to stop any bleeding (have child bite on pad of sterile gauze)
- urgent referral to dental practitioner (child to take tooth/ fragment with them).
The dental practitioner will examine the knocked-out tooth, confirm that the tooth is deciduous and therefore cannot be replaced
It is advisable that any trauma be referred to a dental practitioner as soon as possible. If a permanent tooth is knocked out and is promptly replaced in the socket it has a good chance of survival. Every minute the tooth is out of the socket decreases the chance of the tooth surviving.
What to do if a permanent tooth is knocked out.
- Keep the child calm.
- Locate and retrieve the tooth.
- Handle the tooth by the crown (white part) only, avoid handling the root.
- If root has debris on it, gently rinse the tooth in normal saline or milk. Tap water can be used for a brief rinse if the tooth is visibly dirty and no other option is available.
- Do not attempt to clean the tooth by scrubbing or using cleaning agents.
- Do not let the tooth become dry.
- If the child is conscious: replace the tooth in the socket immediately. You do not need to rinse the socket out. Make sure to put the root into the socket and facing the right way around - look at the other teeth for reference.
- Hold the tooth in place using a small piece of aluminium foil extending across the tooth and its neighbours. The student can also gently hold the tooth with their tongue between their teeth, fingers or bite on a handkerchief or gauze.
If you cannot replace a permanent tooth in its socket (e.g., child can't cooperate) do the following.
- Store the tooth in normal saline, the patients’ saliva or plain milk or wrap the tooth gently in plastic cling wrap to prevent it from drying out. Do not store in water.
- Seek emergency dental treatment immediately as it is important that the tooth be replaced as quickly as possible. The first 30 minutes is critical.
- If an ambulance is called to manage other serious injuries, the package containing the tooth should be well-labelled and accompany the child to the hospital.
6.4 Gingival cysts
Gingival cysts are hard, raised nodules, and are classified as follows:
Epstein’s pearls — are small, white, pearl-like spots that appear in the middle of the hard palate (on the roof of the mouth). These bumps are harmless and tend to disappear within a few weeks.

Bohn’s nodules — are harmless remnants of the dentinal lamina and occur on the labial (cheek side) of the maxillary alveolar ridges (gum ridge). These small, whitish bumps or cysts look like Epstein’s pearls, but can be differentiated by their site of presentation. They are completely benign and disappear on their own within a few weeks to months.

Prevalence
Gingival (keratin) cysts are relatively common in newborns. Epstein’s pearls occur in 60–85 per cent of newborns (Eichenfield & Larralde 2004). Bohn’s nodules occur in up to 85 per cent of newborns (Eichenfield & Larralde 2004).
Causes
Epithelial remnants trapped along lines of fusion of embryological processes.
Age
Usually occur in newborns.
Duration
Nodules usually slough off in the first three months.
Treatment
No treatment is required other than the reassurance of parents
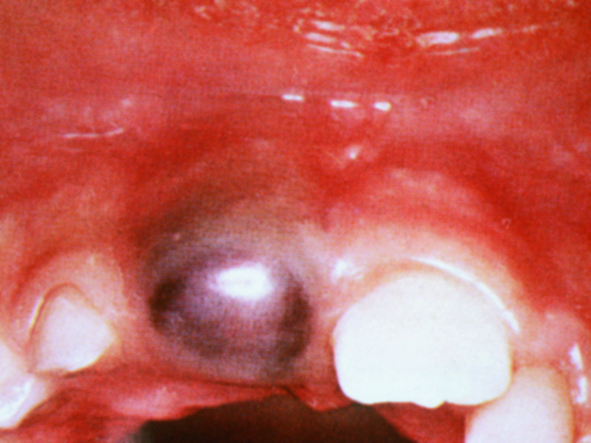
6.5 Eruption cysts
An eruption cyst occurs above an erupting tooth (deciduous and permanent teeth).
Prevalence
Relatively common (Koch, Kreiborg & Andreasen 2009).
Signs and symptoms
An eruption cyst appears as a smooth, localised, dome shaped, fluid filled swelling. It is bluish in colour if it contains blood, is painless and overlies an erupting tooth.
Causes
The cyst is caused by abnormal follicular enlargement just before eruption. Trauma leads to bleeding within the follicle, producing the purplish brown appearance.
Age
Children aged between six months and 12 years.
Duration
The cyst drains once the tooth erupts; this length of time varies from individual to individual. However if it does not resolve within a couple of weeks refer to a dental professional as more serious but very rare conditions can present the same.
Treatment
Usually, no treatment is necessary unless the cyst becomes infected. In this case, a referral to a dental practitioner is required.
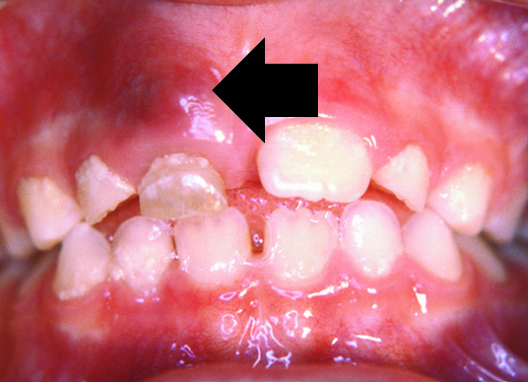
6.6 Dental abscess
A periapical abscess is caused by the spread of infection from the dental pulp (tooth nerve) to the periapical area - the area around the tooth root apex. The abscess may track through to the gingival mucosa where it forms a draining sinus.
Prevalence
A periapical abscess is the most common tooth-related abscess in children (Harris 2008).
Signs and symptoms
There may be a dull throbbing pain associated with the abscess. This pain may be worse while eating or at night. Pus may be visible. A draining sinus associated with an abscess generally appears as a pimple on the gum around the affected tooth.
Causes
A dental abscess is caused by an infection around the root of a tooth. The source of the infection is usually dental caries that has spread to the pulp and then to the periapical area.
Age
All ages of people with teeth.
Duration
A dental abscess will last until definitive treatment is performed. If asymptomatic (shows no noticeable symptoms), a dental practitioner may decide to delay treatment.
Treatment
The child should be referred to a dental practitioner so the tooth can be treated. Treatment depends on which tooth is involved and the extent of the abscess. It may require extraction or root canal treatment. A long-standing abscess on a deciduous tooth can affect the development of the permanent tooth.
6.7 Facial cellulitis
Cellulitis is an acute spreading infection and inflammation of the dermis and connective tissues deep to the dermis, resulting in pain, redness, swelling, and warmth.
Image retrieved from: Oral Health Division, Ministry of Health Malaysia (2017) Clinical Practice Guidelines: Management of Acute Orofacial Infection of Odontogenic Origin in Children (1st ed). Ministry of Health Malaysia, Putrajaya.
Prevalence
Facial cellulitis is more common in children under the age of three (Micali & Dhawan 2010), but can also occur in adults following spreading infection from a grossly carious tooth.
Signs and symptoms
The infection commonly occurs in the facial planes of the lower jaw and is associated with swelling, redness, and inflammation. The patient may display systemic signs of fever.
Causes
Cellulitis is a bacterial infection most commonly caused by Staphylococcus aureus (Staph) or Group A beta haemolytic streptococcus. It has the same underlying causes as an abscess; however, in cellulitis the bacteria spread more widely through the soft tissues. This can occur when a child’s ability to fight infection is reduced or when the bacteria involved are particularly virulent.
Dental caries can lead to infection in the periapical area (around the tooth root). If this infection extends into the surrounding connective tissues, it can cause marked inflammation, swelling, and systemic symptoms such as fever and toxaemia. When this happens, facial cellulitis may develop.
Cellulitis of the head and neck must always be treated promptly, as complications can be serious and potentially life threatening. Referral to an oral health or medical professional is essential. In some cases, the infection can spread to the floor of the mouth and into the pharynx and larynx. This severe condition, known as Ludwig’s angina, can obstruct the airway and requires urgent medical attention.
Age
All age groups.
Duration
Cellulitis is not self limiting, and will last until appropriate treatment is provided.
Treatment
Cellulitis should always be treated with urgency. Management depends on location and extent of swelling and ability to adequately remove the source of infection. Severe cases may require hospitalisation, antibiotics, fluid replacement and removal of the cause, for example, extraction or endodontic (root canal) treatment of the tooth.
6.8 Geographic tongue
Also known as benign migratory glossitis or wandering rash of tongue.

Image sourced from DermNet
Prevalence
Affects approximately 1-2% of the population.
Signs and symptoms
The condition is usually asymptomatic, but it may be associated with sensitivity to acidic foods. Geographic tongue makes the tongue appear patchy. It is characterised by single or multiple areas of pink to red smooth patches where the taste buds appear to be absent, with raised white borders. The areas continually change position and migrate from site to site. Geographic tongue is benign.
Causes
Unknown, but emotional stress, nutritional deficiencies and hereditary factors have been suggested.
Age
Young children to middle-aged adults.
Duration
May appear suddenly and persist for months or years. It often recurs.
Treatment
It is a benign condition and generally does not require any treatment.
6.9 Mucoceles
A mucocele is a cyst-like swelling caused by saliva build-up within subcutaneous tissue following damage to salivary ducts.

Image sourced from DermNet
Prevalence
A mucocele is the most common nodular swelling of the lower lip.
Signs and symptoms
These swellings are asymptomatic, soft, fluctuant, bluish grey (although long standing lesions may have a whitish appearance) and are usually less than one centimetre in diameter. Saliva builds up in connective tissue, which is surrounded in a fibrous capsule. The most common location is the lower lip.
Causes
Arises from trauma to one of the minor salivary glands in the lips or cheeks. Often caused by lower-lip biting or other minor injuries.
Age
Can occur at any age. Children and young adults are mostly affected.
Duration
Superficial lesions usually burst and heal within three to six weeks, they may reform as the tissue fills with saliva again. Persistent lesions require treatment for resolution.
Treatment
Superficial mucoceles usually burst and heal spontaneously. Persistent mucoceles are treated by surgical excision.
The development of a bluish swelling after trauma is suggestive of a mucocele; investigation by a dental practitioner is suggested to exclude other lesions.
6.10 Mouth ulcers
Ulcers can be classified as aphthous, traumatic, herpetic or malignancy.

Image sourced from DermNet
Prevalence
Approximately 20 per cent of the general population is affected by Aphthous ulcers (Vucicevic Boras & Savage 2007). They usually first appear in childhood or adolescence (Scully 2006).
Signs and symptoms
Aphthous ulcers are characterised by painful, recurrent solitary or multiple lesions or ulcerations. They are usually less than five millimetres in diameter. Aphthous ulcers can occur in any site in the mouth, especially on the cheeks, lips and tongue.
Causes
Complex; predisposing factors may include genetics, trauma, tobacco, certain medications, iron/ Vit B12/ folic acid deficiencies, Coeliac disease/ inflammatory bowel disease, sodium lauryl sulphate in toothpaste, hormonal changes, stress (Preeti L et al 2011).
Age
They usually first appear in childhood or adolescence, but can occur in people of all ages.
Duration
Usually heal spontaneously in one to two weeks.
Treatment
No definitive curative treatment. Identify and address any systemic associations. Various topical and systemic agents available. Otherwise provide symptomatic relief.
Symptomatic relief only.
Mouth lesions may be uncomfortable or painful and interfere with eating and drinking. Maintain good oral hygiene – extra care may be required around ulcerated area. Use soft cloth to wipe teeth, if unable to brush. Rinse mouth with salt water (1 tsp salt into 1 cup warm water) a few times/day. Avoid mouthwashes that contain alcohol.
Avoid foods and drinks that will aggravate the lesion. Acidic or spicy (e.g., orange juice, vinegar). Salty (e.g., Vegemite) or very hot. Choose soft/er foods (e.g., jelly, custard) and cool drinks (a straw may help).
Allow the ulcer to heal – do not touch it. Keep hydrated with water and other fluids. Paracetamol can ease pain and fever. Over the counter preparations may be suitable for temporary relief, particularly before eating.
Any ulcer that does not heal within two weeks should be investigated by a medical or a dental practitioner.
Traumatic ulcer
A traumatic ulcer may be the result of:
- mechanical trauma caused by a sharp object (such as a pencil)
- cheek biting
- thermal trauma (such as eating overheated foods or drinks)
- chemical trauma (such as holding aspirin against the oral mucosa).
These ulcers usually heal within a week to 10 days.
Herpetic ulcer (infectious ulcers)
If multiple lesions resembling aphthous ulcers occur accompanied by a fever, malaise, general mouth soreness and inflamed gingivae, an infection with the herpes simplex virus must be considered. This is often seen in babies and young children (see Section 6.12, primary oral herpes simplex infection).
Malignancy ulcer
The most significant of these is caused by leukaemia. These ulcers appear as swelling and ulceration of the gingivae with spontaneous bleeding. Squamous cell carcinoma may present as a discrete ulcer with a characteristic rolled edge, but would be very rare in a child
6.11 Oral candidiasis
Oral candidiasis (thrush) is an overgrowth of oral candida albicans. Candida albicans is a yeast-like fungus that is present in many foods and is part of the normal microbial flora that live in the mouths of around half the Australian population.

Image sourced from DermNet
Prevalence
Relatively common; often seen in babies or infants, or individuals on long term antibiotics or immuno-suppressive drugs
Signs and symptoms
The yeast affects the superficial layers of the mouth tissues. Thrush is generally a local surface infection that produces milky white patches in the mouth. If these patches become dislodged, an erythematous or bleeding surface may be visible beneath them. Oral infection may be associated with infection in the nappy area. Very rarely, fever and gastrointestinal irritation may accompany the disorder, and this signifies a more general infection.
Causes
Overgrowth of candida albicans. Candidiasis can be caused by inhaled cortico-steroids used to treat asthma. Parents should rinse children’s mouth with water after inhalation to reduce the likelihood of infection.
Age
Candidiasis commonly occurs in young babies and infants.
Duration
Infection can persist for days or weeks.
Treatment
Treatment involves assessing the baby and breastfeeding mother, providing advice on minimising reinfection (e.g., sterilising feeding or pumping equipment), and using topical antifungal agents as prescribed by a GP
6.12 Primary oral herpes and simplex infection
The primary form or initial contact of the herpes simplex viruses (types one and two) within the oral cavity may be mild and unnoticed. Some cases can result in extensive oral ulceration involving most of the oral surfaces.



Prevalence
The herpes simplex infection is very common. Around 70 to 90 per cent of adults have herpes simplex antibodies in their bloodstream, which means that they have been infected with the virus at some time (Better Health Channel 2024). People are usually infected in childhood or young adulthood.
Signs and symptoms
Localised inflammation and blistering on the skin. Intra-oral infection may cause vesicles to form, which then burst to cause painful ulceration of the oral mucosa. Infection may be associated with:
- intensely red gums
- gingivitis
- swollen lymph glands
- fever
- restlessness
- bad breath
- dribbling
- dehydration.
Children generally feel unwell or irritable, may have a fever, and are not interested in eating (due to mouth discomfort).
Causes
The initial contact of the herpes simplex viruses (Types 1 and 2) within the oral cavity.
Following this primary infection, the child generally develops immunity, and future infections appear as local lesions (e.g., a discrete cold sore).
Usually transmitted to the child by a parent, relative or friend who has active cold sores when kissing the child.
Age
This primary form of infection usually occurs before the child is five years of age.
Duration
Herpes usually heals within 10 to 14 days.
Treatment
HSV in neonates should be treated as a medical emergency. Urgent referral to hospital is recommended.
In other babies under 3 months, assess for fever, dehydration, poor feeding, or lethargy and refer to a GP due to the risk of serious complications.
6.13 Recurrent herpes simplex and herpes labialis

Image sourced from DermNet
Prevalence
Occur in 40% percent of people who have the initial herpes virus.
Signs and symptoms [Text Wrapping Break]
Recurrent lesions can occur on any site but are more common on the face. The lips are most commonly affected, but infections can occur within the mouth, nose and eyes. The virus causes many painful blisters, which break down to form a collection of ulcers, which can take up to 14 days to disappear.
When they appear on the lips they are commonly referred to as cold sores. The child generally develops immunity after the onset of the primary infection and thereafter develops local lesions (a discreet cold sore). The infected child may suffer fever, malaise and irritability. Small clusters of vesicles rapidly erupt in the mouth and the gums will be very red and swollen and bleed if they are touched. When the vesicles burst, they form yellowish ulcers surrounded by a red halo. Joining of adjacent lesions forms large ulcers in the mouth including the lips and tongue.
Following the original infection, people may suffer from recurrent bouts. Recurrent herpes simplex tends to produce small clusters of vesicles that erupt and form slightly depressed, yellow-brown ulcers that have distinct red halos. Most people report symptoms such as tingling, throbbing and burning one to 24 hours before the eruption of the lesions.
Causes
Herpes-simplex virus. Virus may become active as a result of trauma to the skin and lips (strong sunlight, cold or wind); or being run-down/ stressed/ tired/ unwell.
Age
Any age, following initial infection.
Duration
Lesions can last seven to 14 days.
Treatment
Taking a Lysine supplement orally when the prodromal symptoms appear can prevent the cold sore from developing.
Applying antiviral creams or anesthetic ointments directly to the affected areas can help. Antiviral creams work best when applied early during the prodromal phase.
6.14 Hand, foot, and mouth disease – oral manifestation


Image sourced from DermNet
Prevalence
Hand, foot and mouth disease occurs worldwide, sporadically and in epidemics. It is more common in summer and early autumn. Outbreaks occur frequently among groups of children in childcare centres and schools (Department of Health 2024).
Signs and symptoms
Characterised by numerous shallow painful ulcers in the anterior mouth and on the hands and feet. Most children complain of a sore throat or mouth and may refuse to eat. A low grade fever lasting one to two days is accompanied by a distinctive pattern of oral vesicles and peripheral small flat blisters on the hands and feet, and occasionally on the buttocks. Hand, foot and mouth disease is mild and self-limiting.
Causes
Hand, foot and mouth disease is a symptom of the Coxsackievirus.
Age
Occurs mainly in children under 10 years and in young adults.
Duration
- Low-grade fever lasts 1-2 days accompanied by a distinctive pattern of oral vesicles, mainly on the tongue and buccal mucosa (also lesions on the hands and feet, and occasionally buttocks).
- Ulceration lasts 7-10 days.
Treatment
It is recommend child see a medical practitioner
Symptomatic relief only
Mouth lesions may be uncomfortable or painful and interfere with eating and drinking. Maintain good oral hygiene – extra care may be required around ulcerated area. Use soft cloth to wipe teeth, if unable to brush. Rinse mouth with salt water (1 tsp salt into 1 cup warm water) a few times/day. Avoid mouthwashes that contain alcohol.
Avoid foods and drinks that will aggravate the lesion. Acidic or spicy (e.g., orange juice, vinegar). Salty (e.g., Vegemite) or very hot. Choose soft/er foods (e.g., jelly, custard) and cool drinks (a straw may help).
Allow ulcer/s to heal – do not touch. Keep hydrated with water and other fluids. Paracetamol can ease pain and fever.
6.15 Measles -oral manifestation

Prevalence
Not endemic in Australia; cases still occur due to importation by overseas travelers.
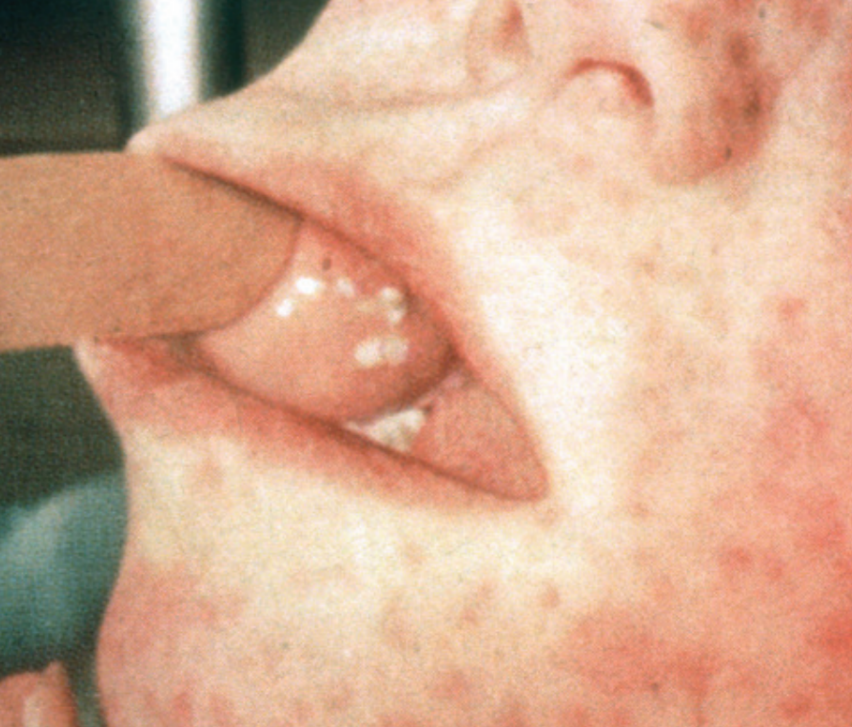
Signs and symptoms
Measles can be identified by the presence of characteristic mouth lesions called Koplik’s spots. They are small white spots (like grains of salt) surrounded by a zone of inflammation and are often numerous on the inside of the cheeks or around the upper salivary duct in the upper cheek area. Koplik’s spots appear about two to three days before the general rash and coincide with the most infectious period. They disappear with the development of the general skin rash that usually starts behind the ears and spreads down over the face and body. It consists of purplish or red raised spots that run together to form blotchy areas. Red eyes and a dry cough can also be features.
Causes
Measles is caused by the measles virus (paramyxovirus).
Age
Infants and children are especially vulnerable. Anyone at any age can be affected if not immune
Duration
Incubation period is approximately ten days but varies from seven to ten days from exposure to the onset of fever. It is usually 14 days until the rash appears.
Treatment
MCH nurses will already be aware that measles is a nationally notifiable disease that must be reported to the Department of Health.
Because of the risk of complications, referral to a medical professional is required. The child should have an isolation period of at least five days from the appearance of the rash. The treatment is similar to that of fever, and involves analgesia for fever, and providing fluids and a soft diet.
6.16 Tongue tie (ankyloglossia)
Tongue ties are caused by a short frenum that restricts tongue movement.

Signs and symptoms
Most babies with tongue tie breast and bottle feed successfully, but a tight tongue tie can interfere with a baby’s ability to breastfeed and, in some cases, bottle feed.
The symptoms of tongue tie can include:
- tongue can’t poke out past the lips
- tongue tip can’t touch the roof of the mouth
- tongue can’t be moved sideways to the corners of the mouth
- tongue tip may look flat or square, instead of pointy when the tongue is extended
- tongue tip may look notched or heart shaped
- may have breastfeeding or bottle-feeding problems
- the front teeth in the lower jaw may have a gap between them.
Tongue tie can be hard to diagnose in newborns. It is important for a mother to consult with a medical professional or lactation consultant if they are having trouble breastfeeding. Signs that a baby could be tongue tied include:
- mother has sore nipples during and after breastfeeding
- mother has squashed nipples after breastfeeding
- mother has a white compression mark on the nipple after breastfeeding
- the baby has difficulty latching on to the nipple
- the baby often loses suction while feeding and sucks air
- the baby’s mouth makes a clicking sound while feeding
- the baby fails to gain weight.
Causes
There are two main causes of tongue tie: either the frenum is too short and tight, or it failed to move back down the tongue during development and is still attached to the tongue tip. In the second case, a heart-shaped tongue tip is one of the obvious symptoms. It is not clear whether or not tongue tie is inherited.
Age
Tongue tie is congenital, but may not be noticed until the child has trouble eating or speaking.
Duration
Tongue tie can resolve in early childhood if the frenum loosens by itself, allowing the tongue to move freely for eating and speech. In some cases the child may need to have an operation (frenectomy) to release the tongue.
Treatment
The preferred treatment is to wait to see if the tongue tie resolves spontaneously.
Parents and babies experiencing feeding problems should see a lactation consultant or feeding specialist to confirm whether or not the tongue tie is related the feeding problem as there are many causes of difficulty breast feeding.
Toddlers or older children should see a speech therapist to work out whether the tongue tie is causing the speech or eating problems.
6.17 Cleft lip and palate


Prevalence
About 1 in 800 babies born in Australia
Signs and symptoms
A cleft palate may lead to feeding problems, as the child is unable to achieve the suction necessary to draw the milk. When babies with cleft lip and/or palate feed they may:
- feed slowly
- cough and splutter during feeding
- become windy and need to be burped more frequently
- have milk escape from their nose during feeding (nasal regurgitation), especially if the flow of milk from the teat is fast
- fail to gain appropriate weight for age.
Cause
Abnormal foetal development where the tissues of the lip, upper jaw or the roof of the mouth fail to fuse properly
Age
While a cleft lip and/or palate is apparent at birth, a cleft palate may be overlooked until other signs and symptoms are present.
Treatment
- Referral to a paediatrician is required if a previously undiagnosed cleft palate is suspected.
- The amount of treatment required for a child with a cleft lip or palate depends on a range of factors, and severe defects do not always require complex treatment.
- Depending on the case, a range of specialists may be required, including audiologists, dental specialists, ear, nose and throat surgeons, oral and maxillofacial surgeons, paediatricians, plastic surgeons and speech pathologists